Spanish
Spanish  Chinese
Chinese  Russian
Russian  German
German  French
French  Japanese
Japanese  Portuguese
Portuguese  Hindi
Hindi Opinion Article, Int J Glob Health Vol: 8 Issue: 1
Trauma-Induced Coagulopathy: Diagnostic Challenges and Therapeutic Strategies
Ronald Chang *
Department of Surgery, University of Texas, Houston, United States of America
*Corresponding Author: Ronald Chang,
Department of Surgery, University of Texas, Houston, United States of America
E-mail:ronald.ch@tmc.edu
Received: 16 August, 2024, Manuscript No. IJGH-24-145574;
Editor assigned: 20 August, 2024, PreQC No. IJGH-24-145574 (PQ);
Reviewed:03 September, 2024, QC No. IJGH-24-145574;
Revised: 14 February, 2025, Manuscript No. IJGH-24-145574 (R);
Published: 21 February, 2025, DOI: 10.4172/Ijgh.1000224.
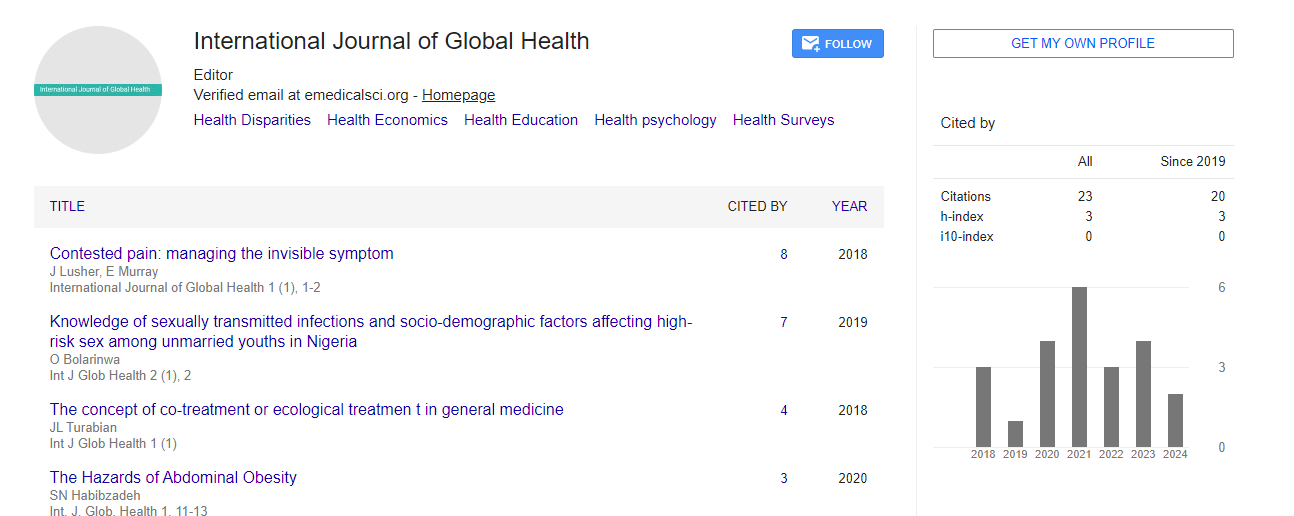
Citation: Chang R (2025) Trauma-Induced Coagulopathy: Diagnostic Challenges and Therapeutic Strategies. Int J Glob Health 8:1.
Introduction
Trauma-Induced Coagulopathy (TIC) is a complex condition characterized by abnormal blood clotting following severe trauma. It contributes to increased morbidity and mortality in trauma patients. This manuscript explores the pathophysiology of TIC, the challenges of early diagnosis, and the evolving strategies for its management. Recent advances in understanding the mechanisms behind TIC, such as endothelial injury, hypoperfusion, and inflammation, have led to the development of targeted interventions. This review highlights the importance of early recognition and appropriate management of TIC to improve outcomes in trauma patients.
Trauma-Induced Coagulopathy (TIC) is a significant complication in patients suffering from severe trauma and is associated with increased morbidity and mortality. TIC is characterized by an inability to maintain hemostasis, leading to excessive bleeding, organ dysfunction, and poor outcomes. It is a multifactorial condition influenced by factors such as hypoperfusion, acidosis, inflammation, and endothelial injury.
Pathophysiology of trauma-induced coagulopathy
TIC is a dynamic process that begins immediately after trauma and evolves over time. Several interrelated factors contribute to the development of TIC, including:
Endothelial dysfunction
Endothelial injury plays a central role in the pathogenesis of TIC. Trauma triggers the release of inflammatory cytokines and mediators, leading to endothelial activation and dysfunction. This results in the loss of the normal anticoagulant properties of the endothelium, with subsequent activation of the coagulation cascade.
Endothelial dysfunction also leads to increased permeability, resulting in leakage of plasma proteins and coagulation factors into the extravascular space. Additionally, the release of tissue factor from damaged endothelial cells initiates the extrinsic coagulation pathway, further exacerbating the hypercoagulable state.
Hypoperfusion and acidosis
Hypoperfusion and shock following trauma contribute significantly to the development of TIC. Inadequate tissue perfusion leads to anaerobic metabolism and the accumulation of lactic acid, resulting in acidosis. Acidosis impairs the function of coagulation enzymes, reducing clot formation and stability.
Furthermore, hypoperfusion and acidosis promote the release of tissue Plasminogen Activator (tPA), leading to hyperfibrinolysis–the excessive breakdown of clots. This results in the rapid dissolution of blood clots, contributing to ongoing hemorrhage and worsening coagulopathy.
Inflammation and immune response
The systemic inflammatory response to trauma plays a critical role in TIC. The release of pro-inflammatory cytokines, such as Tumor Necrosis Factor-alpha (TNF-α) and interleukins, activates the coagulation system and promotes endothelial injury. At the same time, the immune response can lead to the consumption of coagulation factors and platelets, further impairing hemostasis.
Inflammation also triggers the release of microparticles and extracellular vesicles, which can activate the coagulation cascade and promote thrombin generation. The resulting hypercoagulable state is often followed by a secondary phase of hypocoagulability, where the consumption of clotting factors leads to an increased risk of bleeding.
Fibrinolysis dysregulations
TIC is often associated with dysregulation of the fibrinolytic system. Hyperfibrinolysis, driven by the overactivation of tPA, results in the breakdown of fibrin clots and contributes to uncontrolled bleeding. Conversely, hypofibrinolysis, or the inhibition of fibrinolysis, can lead to microvascular thrombosis and organ dysfunction.
The balance between coagulation and fibrinolysis is delicate, and disruptions in this balance are a hallmark of TIC. Identifying and addressing fibrinolysis dysregulation is a critical component of TIC management.
Diagnosis of trauma-induced coagulopathy
Early and accurate diagnosis of TIC is essential for guiding appropriate management. Traditional coagulation tests, such as Prothrombin Time (PT), activated Partial Thromboplastin Time (aPTT), and platelet count, are commonly used but may not fully capture the complexity of TIC. These tests are often too slow to provide real-time information in the acute trauma setting. Point-of- Care Testing (POCT) methods, such as Thromboelastography (TEG) and Rotational Thromboelastometry (ROTEM), have emerged as valuable tools in the early diagnosis and monitoring of TIC. These tests provide a comprehensive assessment of the coagulation process, including clot formation, strength, and stability. They can also detect fibrinolysis abnormalities, guiding targeted interventions.
Biomarkers
In addition to POCT, several biomarkers have been investigated for their potential role in diagnosing TIC. These include markers of endothelial injury (e.g., syndecan-1), fibrinolysis (e.g., D-dimer), and inflammation (e.g., C-reactive protein). While these biomarkers show promise, further research is needed to establish their utility in routine clinical practice.
Management of trauma-induced coagulopathy
Damage Control Resuscitation (DCR) is a key strategy in managing TIC. DCR involves the early and aggressive correction of hypoperfusion and coagulopathy while minimizing further blood loss. Maintaining a lower-than-normal blood pressure to reduce bleeding while ensuring adequate perfusion to vital organs. Early use of blood products, such as packed red blood cells, plasma, and platelets, in a balanced ratio to address coagulopathy.
Avoid excessive crystalloid infusion, which can dilute coagulation factors and worsen coagulopathy. Despite advances in understanding and managing TIC, several challenges remain. One of the key challenges is the variability in TIC presentation among trauma patients, making it difficult to develop standardized treatment protocols. Additionally, the timing and dosing of interventions, such as blood products and hemostatic agents, require further research to optimize outcomes.
Conclusion
Trauma-induced coagulopathy is a complex and life-threatening condition that requires early recognition and targeted intervention. Advances in our understanding of the underlying mechanisms, coupled with the development of point-of-care diagnostic tools and innovative treatment strategies, have improved the management of TIC. However, ongoing research and refinement of current practices are essential to further enhance outcomes for trauma patients.